35 yr old man presented with shortness of breath
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case i have seen:
35 years male Daily wage labourer, married 10 yrs back ,has 2 sons (9yrs,7yrs) used to drink 90 ml /day started at the age of 20yrs , stopped 3yrs back (bcoz of his wife) . Again started from 4 months daily bcoz of his friends (90ml/day).
10 days back he went to a function ,got drunk and had a fall from bike (no h/o loc, vomitings,bleed from ears ,nose; headache, dizziness.) Injury to lateral side of leg by bike silencer 5 x3 cms ulcer .Got treated symptomatically for pain and ulcer dressings in their local area. Yesterday morning 2.00am he went to urinate,but he was not able to pass the urine , developed shortness of breath, orthopnea+, went to nearby hospital ,got relieved for sometime on oxygen therapy.Later he was referred to our hospital. Pt is k/c/o Asthma (on inhaler) from 6months.
Not a k/c/o Dm2/HTN/TB/Epilepsy/CAD
NO H/O Fever,cough, vomitings,loose stools,pedal edema,chestpain, palpitations.
No h/o past surgeries.
On examination:
Patient was conscious, coherent and cooperative.
Vitals:
Patient is afebrile
Respiratory rate: Tachypneic 35 cpm
Bp: non recordable and immediately started on with dobutamine @4ml / hr.
CVS: S1, S2 heard, no murmurs
Respiratory system:
Bilateral diffuse crepitations heard.
Per abdomen:
Soft, non tender
Bowel sounds heard
CNS: GCS: E4V5M6
No abnormality detected.
Patient suddenly went to cardiac arrest at 5:30 am Emergency resuscitation done but patient died due to cardiopulmonary arrest with reduced ejection fraction( EF- 40%).
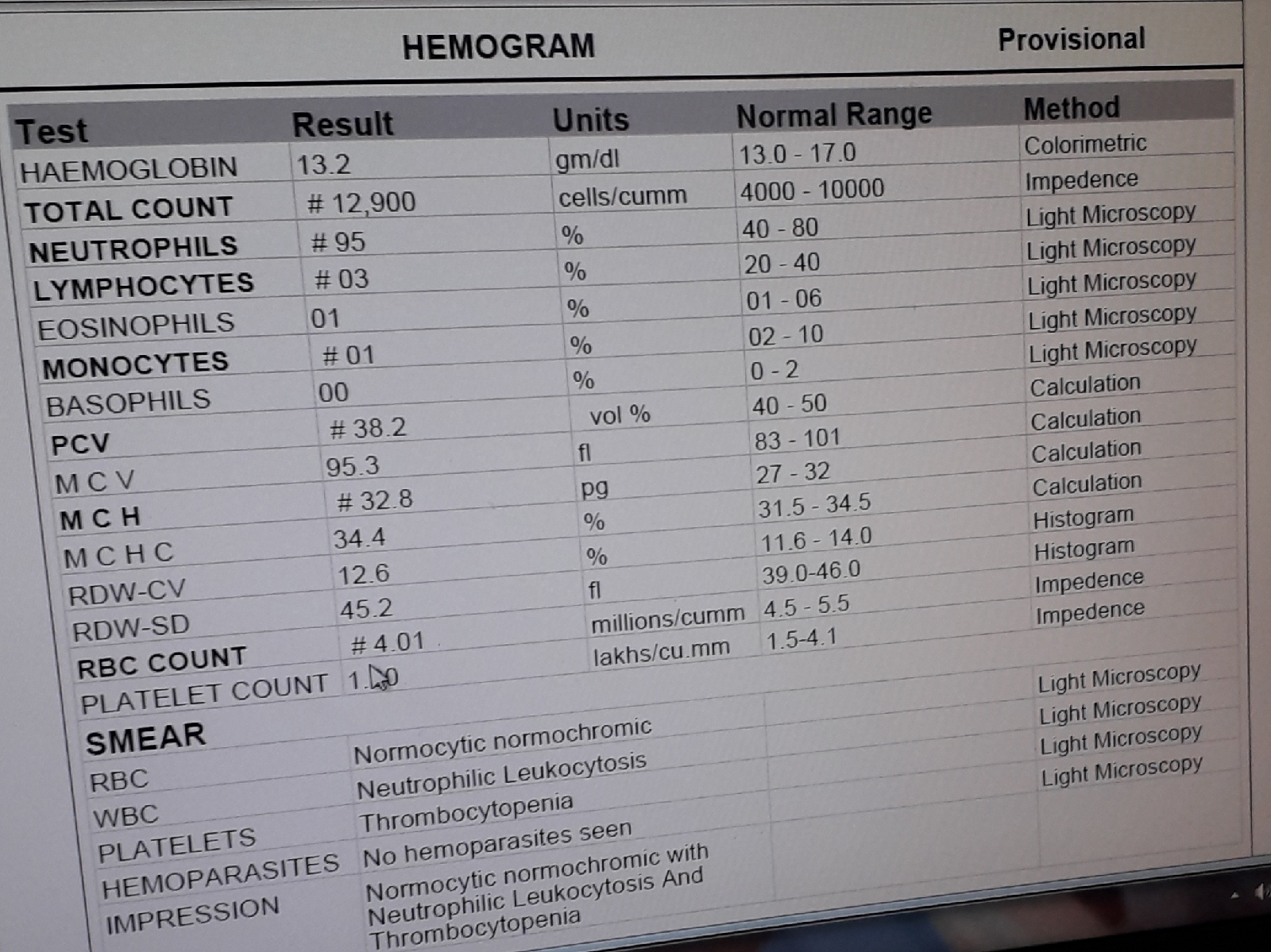
Investigations













Treatment
Inj dobutamine IV infusion at the rate of 4 ml / min
Inj noradrenaline IV infusion at the rate of 6 ml /min
Inj piptaz 4.5 gm iv stat
Inj pan 40 mg IV BD
Inj lasix 40 mg IV if SBP is greater than 120 mm hg
BP,PR ,RR ,SPO2 monitored hourly


{kind=link}
{kind=link}
{kind=link}